
Yet to conceive? It could be a case of PCOS
In my related years of practice in the realm of diagnostic medicine, I have come to realise that unbeknown to many, one medical condition that is commonly overlooked in women in reproductive-age group, especially those who have issues with getting pregnant, is Polycystic ovary syndrome (PCOS). It is one of the commonest female blood-chemicals regulatory (endocrine) disorders affecting approximately one-sixth of women of reproductive age i.e. 12–45 years old, and by inference one of the leading causes of female subfertility.
Beyond the concurrent issue of inability to conceive, PCOS is a spectrum of medical conditions, which has as its principal features conditions like obesity, unpredictable ability to produce and release matured eggs (anovulation), which may result to irregular menstruation or lack of menses (amenorrhea), acne, and excessive amounts of androgenic (male characters-enhancing) hormones manifesting as male hair pattern on the face/pubic area.
On severity scale, the manifestations of PCOS vary greatly among women, while in some the features are mild, in others it comes in full blown in its manifestation. Although, the causes are unknown, obesity, insulin resistance and diabetes are known to occur recurrently with PCOS.
A typical PCOS storyline is that of my recent encounter with Tonia, 34 years old lady, married to Niyi, 37 years old. They have been married for five years with not history of conception. Tonia is moderately obese, with recurrent issue of lengthy menstrual cycle beyond 34 days and she sometimes missed her menses many months over without testing positive on pregnancy test.
Initial assessment on ultrasound scan showed that Tonia has normal reproductive organs (aside multiple small cysts seen in the ovaries) while sono-contrast test also confirmed normal opening of the (fallopian) tubes which connect the womb and the eggs’ center (ovary) on either side. These findings showed that Tonia’s fertility issue is not primarily structural but most probably a functional (endocrine-related) issue; thus putting an instant spot on Tonia as an incidental case of polycystic ovary syndrome.
Further curious assessment carried on Tonia revealed that her blood sugar level was very much on the high side at 300mg/dl (well above the normal reference point of 126mg/dl).
How it occurs
Polycystic ovaries develop when the ovaries are stimulated to produce excessive amounts of male hormones (androgens), particularly testosterone, either through the release of excessive luteinizing hormone (LH) by the anterior pituitary gland or through high levels of insulin in the blood (hyperinsulinaemia) in women whose ovaries are sensitive to this stimulus.
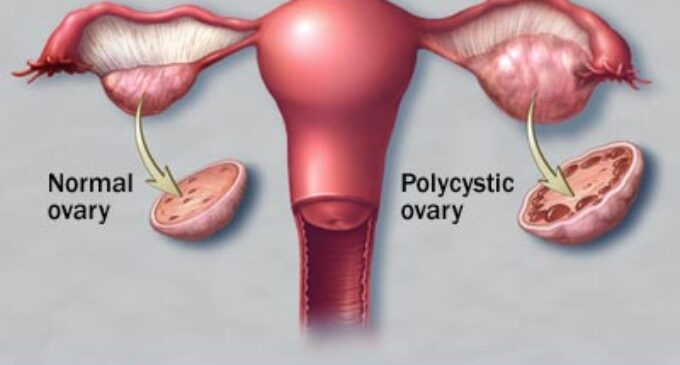
The syndrome acquired its most widely used name due to the common sign on ultrasound examination of multiple (poly) ovarian cysts (though not given in all “PCOS” cases). These “cysts” are actually immature follicles, not cysts in the context of their sizes. The follicles have developed from primordial follicles, but the development has stopped (“arrested”) at an early stage due to the disturbed ovarian function. The condition was first described in 1935 by Dr. Stein and Dr. Leventhal, hence its original name of Stein-Leventhal syndrome.
As noted above, majority of patients with PCOS have insulin resistance and/or are obese. Their elevated insulin levels contribute to or cause the abnormalities seen in the hypothalamic-pituitary-ovarian axis that lead to PCOS.
The prevalence of PCOS has increased with the use of different diagnostic criteria and has recently been shown to be 18% (17.8 ± 2.8%) in the first community-based prevalence study based on current diagnostic criteria. Importantly, 70% of women in the aforementioned study were undiagnosed PCOS cases.
Signs and symptoms
Common symptoms of PCOS include
- Menstrual disorders – mostly haphazard periods or lack of menses over a longtime without being pregnant.
- Infertility, generally resulting from chronic lack of ovulation.
- Hirsutism (male-like hair pattern in a woman), and/or symptoms of hyperandrogenism, such as recurrent and persistent pimples.
- Metabolic syndrome, characterised by central obesity, insulin resistance (feature of diabetes) and other symptoms.
PCOS can present in any age during the reproductive years. Due to its often vague presentation it can however take years to reach the diagnosis.
Diagnosis
However, one thing to note is that not all women with PCOS have polycystic ovaries (PCO), nor do all women with ovarian cysts have PCOS; although a pelvic ultrasound is a major diagnostic tool, it is not the only one. Standard diagnostic assessments include:
History-taking, specifically for menstrual pattern, obesity, hirsutism, and the absence of breast development. A clinical prediction rule found that these four questions can diagnose PCOS with a sensitivity of 77.1% and a specificity of 93.8%.
Gynecologic ultrasonography, specifically looking for small ovarian follicles are believed to be the result of disturbed ovarian function with failed ovulation, reflected by the infrequent or absent menstruation that is typical of the condition.
In normal menstrual cycle, one egg is released from a dominant follicle – essentially a (fluid-filled) cyst that bursts to release the egg. After ovulation the follicle remnant is transformed into a progesterone-producing corpus luteum, which shrinks and disappears after approximately 12–14 days. In PCOS, there is a so called “follicular arrest”, i.e., several follicles develop to a size of 5–7 mm, but not further. No single follicle reached the preovulatory size (16 mm or more). According to the diagnostic criteria, 12 or more small follicles should be seen in an ovary on ultrasound examination. The follicles may be oriented in the periphery, giving the appearance of a ‘string of pearls’. The numerous follicles contribute to the increased size of the ovaries often seen in PCOS cases, that is, 1.5 to 3 times larger than normal.
Laparoscopic examination may reveal a thickened, smooth, pearl-white outer surface of the ovary.
Serum (blood) levels of androgens (male hormones), including androstenedione, testosterone etc is higher than normal. The free testosterone level is thought to be the best measure, with ~60% of PCOS patients demonstrating the aforementioned supranormal levels.
Aside the routine fasting blood sugar mentioned earlier, patient with equivocal FBS reading often test high to a 2-hour oral glucose tolerance test (GTT) especially in those with risk factors (obesity, family history, history of gestational diabetes), which indicate impaired glucose tolerance (insulin resistance) in some women with PCOS. Frank diabetes can be seen in 65–68% of women with this condition. Insulin resistance can be observed in both normal weight and the obese.
Treatment of Polycystic Ovarian Syndrome
Treatment of PCOS is tailored to the patient’s goals. Broadly, these may be considered under four categories:
- Lowering of insulin levels
- Restoration of fertility
- Restoration of regular menstruation, and prevention of endometrial hyperplasia and endometrial cancer
- Treatment of excessive body hair growth in the woman (hirsutism) or acne
General interventions that help to reduce weight or insulin resistance can be beneficial for all these aims, because they address what is believed to be the underlying cause.
Diet helps
Where PCOS is associated with overweight or obesity, successful weight loss is probably the most effective method of restoring normal ovulation/menstruation, but many women find it very difficult to achieve and sustain significant weight loss. Low-carbohydrate diets and sustained regular exercise may help. Some experts recommend a low GI diet in which a significant part of total carbohydrates are obtained from fruit, vegetables and whole grain sources.
Drugs use
Reducing insulin resistance by improving insulin sensitivity through medications has been an obvious approach that comes handy with the use of relevant anti-insulin resistance medications.
Treating infertility
Curious enough, not all women with PCOS have difficulty becoming pregnant. For those who do, anovulation is a common cause; inferably, the presence of ovulation ordinarily indicates absence of infertility, although it does not rule out infertility by other causes.
For overweight women with PCOS, who are anovulatory, diet adjustments and weight loss could result to resumption of spontaneous ovulation.
In those who after weight loss are still anovulatory or for anovulatory lean women, then relevant prescription medication can come handy.
For patients who do not respond to drugs, diet and lifestyle modification, there are options available including assisted reproductive technology procedures such as controlled ovarian hyperstimulation with follicle-stimulating hormone (FSH) injections followed by in vitro fertilisation (IVF) etc.
Surgery may help
Though surgery is not commonly performed, the polycystic ovaries can be treated with a laparoscopic procedure called “ovarian drilling” (puncture of 4-10 small follicles with electrocautery), which often results in either resumption of spontaneous ovulations or ovulations after adjuvant treatment with clomiphene or FSH.
The ultimate message here, especially in the ‘not-so-straight-forward’ cases of infertility, it may be important to “scope” further, in order to rule out convincingly that a case of polycystic ovary syndrome (PCOS) is not being overlooked.
*Dr Akinrogunde is principal associate, GTAK Health Communication and Allied Services










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Very informative. Thank you Dr.
Thanks, Dr.very informative
Very interesting read … I have PCOS for years and discovered it very early. I have had 2 kids and getting pregnant was a challenge but with A Prescription drug- Clomid I was able to ovulate and get pregnant. I now take Another Prescription drug- Metformine, excercise and diet to prevent diabetes. Thanks once again.
I am very happy to read this article. My wife was on Cs in 2007 one week after she came up with the sign of anaemia after given her blood , she bleeds and she was given another one. For several times she received and several times she bleeds. At the end, God help the blood stopped. Since then, she has not seen her mensturation almost seven years known. pls help.
Polycarp,
Nice knowing my piece was worth the while. We can review your wife’s case together, write me on [email protected]
Dr Goke
Nice one DR Goke. Am so so glad we have a consultant like you here in Nigeria that have taken time to study this case PCOS. This is so so timely for me. God bless you sir.